
Wednesday morning arrives and we are ready to take on the day.
The ankle case is posted. I think I discussed her situation briefly. In summary, this lady had an ankle fusion approximately 3-4 months ago. After her initial surgery, she suffered a fracture of the tibia above the level of the ankle fusion. The fracture fell into valgus creating a malunion. Matt, Natalie, and I (along with online chat advice from other surgeons) have discussed multiple options to correct the deformity trying to take into account the implant and equipment limitations we face here.
I must take a moment to praise the lead resident of this case – Dr Johnson Mbise. Dr Johnson is a go-getter and from the beginning has literally hounded us about booking these deformity corrections and is very enthusiastic to partake in discussion and participate in surgery. He is quiet and unassuming but when given time, he has a nice collection of orthopedic knowledge and questions. It is a resident like Dr Johnson that proves the goals of this trip and others are reachable – long term change with education!
Natalie joined an infected femur/hardware removal case done without flouro (X-ray). Perhaps those who know her can pressure her to post on those adventures.
Matt, Johnson, and I got started on the ankle. We were able to take out the previous hardware without using tourniquet or flouro and then began our medial approach to the partially united fracture. While early healing had occurred, we found the old fracture line and created some separation between the fracture edges. Additional release laterally allowed the fracture to be mobilized and swung into the corrected position. In addition, previous CT showed incomplete joint healing at the ankle in the medial aspect. We were able to do some debridement and re-preparation of the joint there.



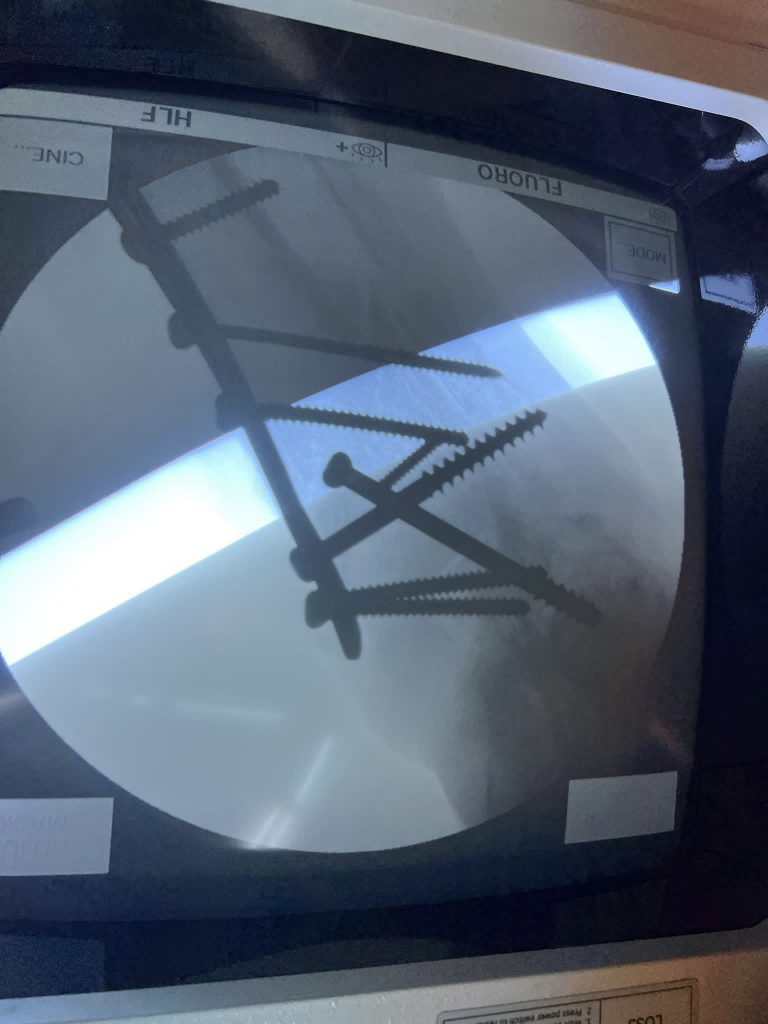
The trial of these cases in this environment comes when the prep work is done and it is time to lock in the correction. Matt had found the plate needed ahead of time, so we were good there. however, all plates need screws and assorted trays were delivered to the table with assorted sizes, thread types, and such for fixation. Rather then asking for a 68mm fully threaded 4.5 screw, we would ask for something between 60-70mm preferably with more threads than fewer. A little creativity goes a long way, and we were able to position and fix the plate/bone without getting the bolt-cutters out to “adjust” screw sizes – always a win in my book!
There’s an old saying that nothing ruins a good case like follow-up – meaning she has a long road to travel to heal, but I think the starting point is a least a satisfactory one. Some pics and xrays are below.
PS – for the foot and ankle/trauma folks out there, we wanted to put in a nail, but this was largely overruled by a local staff who felt this was not a good idea. We also had concerns about the ability to place the nail well with the x-ray limitations currently in the OR – flouroscopy does not work well if moved! But no worries, we are going to try a nail for next week’s Charcot ankle correction. (If that paragraph means nothing to you, I sum it up by saying pray for us during that case!)



2 responses to “A crooked staff can’t cast a straight shadow”
I have to thank you for the efforts you’ve put in writing this blog. I’m hoping to view the same high-grade blog posts from you in the future as well. In truth, your creative writing abilities has inspired me to get my own blog now 😉
Pretty! This has been a really wonderful article. Thanks for providing this info.